SCI论文(www.lunwensci.com):
摘要:目的评估延续性护理干预对血液透析患者抑郁、焦虑和压力负性情绪的影响。方法随机选取了2014年1月至2019年1月在本院接受血液透析的60例晚期慢性肾病患者,分为出院后接受持续电话随访的观察组和只接受住院常规护理的对照组每组30例,干预前两组患者填写第一部分人口统计学调查问卷,经干预后两组患者填写第二部分DASS量表。结果两组患者在社会人口统计学特征方面相似无显著统计学差异(P>0.05);干预前两组患者DASS量表无显著差异(P>0.05);两组患者在干预后观察到DASS量表的评分存在显著差异(P<0.05),观察组的平均得分高于对照组。结论本研究结果有望为血液透析患者的有效随访提供新的理论支持以改善他们的情绪和健康状况,证实了临床专科护士通过延续性护理干预措施在改善血液透析患者心理健康方面的重要性。
关键词:延续性护理;抑郁;焦虑;压力;血液透析患者;慢性肾病;DASS量表
本文引用格式:陈学英,沈瑜,姚小峰,等.延续性护理干预对血液透析患者抑郁、焦虑和压力负性情绪的影响[J].世界最新医学信息文摘,2019,19(71):371-372,374.
Effect of Continuous Nursing Intervention on Depression,Anxiety and Stress Negative Emotion in Hemodialysis Patients
CHEN Xue-ying,SHEN Yu,YAO Xiao-feng,SONG Xiao-li
(Suzhou ninth People's Hospital,Suzhou Jiangsu)
ABSTRACT:Objective To evaluate the effects of continuous nursing intervention on depression,anxiety and stress negative emotions in hemodialysis patients.Methods Sixty patients with advanced chronic kidney disease who underwent hemodialysis from January 2014 to January 2019 were randomLy selected.The observation group was followed by continuous telephone follow-up after discharge and the control group receiving only routine hospital care.Thirty patients were enrolled in the first part of the demographic questionnaire before the intervention.After the intervention,the two groups filled out the second part of the DASS scale.Results There were no significant differences in sociodemographic characteristics between the two groups(P>0.05).There was no significant difference in the DASS scale between the two groups before intervention(P>0.05).The two groups of patients observed DASS scale after the intervention.There was a significant difference in the scores of the scale(P<0.05),and the average score of the observation group was higher than that of the control group.Conclusion The results of this study are expected to provide new theoretical support for effective follow-up of hemodialysis patients to improve their emotional and health status,confirming the importance of clinical nurses in improving the mental health of hemodialysis patients through continuous nursing interventions.
KEY WORDS:Continuous care;Depression;Anxiety;Stress;Hemodialysis patients;Chronic kidney disease;DASS scale
0引言
慢性肾病(Chronic Kidney Disease,CKD)是一种不易发现的疾病,经常在晚期被诊断出来,而血液透析和肾移植是其唯一的治疗选择,透析患者患有多重躯体症状的大负担[1]。慢性肾病患者普遍存在认知障碍和抑郁,接受血液透析的老年患者的焦虑水平高于健康老年人[2],此外焦虑还会降低这些患者的生活质量并延长住院时间[3]。血液透析患者临床抑郁症的平均患病率约为20%~30%,42%的血液透析患者表现出某种类型的抑郁情绪[4,5]。这些比率大大高于一般人群,其中抑郁率在3%~6%之间,而老年人的比率在6%~10%之间[6]。有研究表明,到2050年成年人的抑郁率将增加35%,老年人的抑郁率将增加一倍以上[7]。尽管抑郁症的患病率高达60%,而且具有严重后果。但抑郁仍然是一种容易误诊的疾病,这可能是由于与尿毒症相关的叠加症状(厌食,疲劳,睡眠障碍)以及缺乏系统的精神病学评估[8]。抑郁症治疗的重要性已成为肾脏疾病研究文献的焦点,一些作者[9]建议对抑郁症患者进行筛查并提供适当的护理。然而血液透析患者中大量未确诊和未治疗的抑郁症表明这些患者存在心理保健障碍[10]。已经有研究使用各种方法来减少焦虑症状[11],延续性护理干预模式是住院患者出院后到家庭的持续性和整体性护理模式,其中对患者出院后持续性的电话随访被认为是一种低成本且易于组织的护理干预措施,是管理患者疾病进程、早期识别并发症、保证和优质护理的好方法,同时可进行信息交流和对患者及其家属提供健康教育[12]。本研究旨在评估护士主导的延续性护理干预,主要以电话随访远程护理的方式对本院血液透析患者抑郁、焦虑和压力的影响。
1资料与方法
1.1基本资料
基于双盲随机临床试验选择的研究对象包括60名接受血液透析治疗的晚期慢性肾病患者,选取了2014年1月至2019年1月在本院接受血液透析的患者,分为观察组和对照组,每组30例。纳入标准:①年龄在18~65岁之间;②没有认知和心理障碍;③至少接受过小学教育;④达到肾脏疾病的最后阶段和接受持续性治疗;⑤接受至少6个月的血液透析治疗,每周三次治疗,持续三到四个小时;⑥在干预期间没有肾移植和转院;⑦没有接受血液透析有关的正式培训。排除标准:①在过去六个月内有过严重疾病病史;②接受抗抑郁药物治疗;③因急性疾病住院;④不愿意继续参与研究,中途退出研究。本研究得到本院伦理委员会的批准,在解释研究目标并获得参与者的书面知情同意后进行数据收集。两组患者的基线资料比较无统计学差异P>0.05,可进行比较。
1.2方法与评价指标
调查问卷由患者在延续性护理干预前完成,对照组没有电话随访只接受了医院的常规护理,观察组除常规治疗外在接受血液透析移位后30天接受电话随访。电话随访进行结构化内容咨询,所有延续性护理干预措施均由负责该实验的研究人员进行,每次通话持续30分钟,两组患者在完成研究后填写DASS量表。
由两部分内容组成的调查问卷用于数据收集,第一部分内容包括七个问题,涉及患者的人口统计特征,包括年龄,性别,婚姻状况,就业情况,教育水平,收入水平和一周血液透析频率。第二部分内容是抑郁焦虑和压力量表(DASS),这是一种被广泛使用的筛查工具,用于评估社区环境中患者的抑郁、焦虑和压力的症状。该量表包括三个子量表:(1)抑郁量表,用于测量绝望、自卑和负面情绪;(2)焦虑量表,用于评估自主觉醒、肌肉骨骼症状、情境焦虑和焦虑唤醒的主观体验;(3)压力量表,用于评估紧张、焦虑和情绪激动。DASS有两种形式,即全42项和短21项版本,两者都评估相同的领域。
DASS-21由21个项目组成,每个量表中有7个项目,分别测量当前的抑郁、焦虑和压力症状。DASS-21使用四级量表对严重程度进行评级,范围从0(根本不适用于我)到3(非常适用于我)。为了获得总分和抑郁、焦虑和压力的分数,根据开发该工具的Lovibond[13]的推荐,将各个项目的个体分数相加并乘以2,每个区域的得分范围从0到21。
1.3统计学分析
数据通过SPSS 21.0进行分析,并且还包括描述性和分析性统计,包括独立样本t检验、卡方检验、配对t检验和方差分析,以P<0.05为差异有统计学意义。
2结果
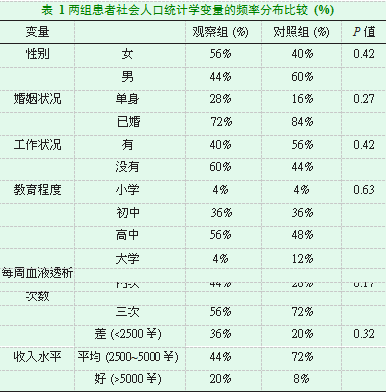
2.1两组患者社会人口统计学变量的频率分布比较
表1显示了两组患者的社会人口统计学特征,参与者的平均年龄为69.13±11.82,经卡方检验表明,两组在社会人口统计学特征方面相似无统计学差异(P>0.05)。
2.2两组患者干预前的抑郁、焦虑和压力评分的平均值比较
表2显示了两组患者干预前血液透析患者的抑郁、焦虑和压力评分的平均值,采用两独立样本t检验,干预前两组患者DASS量表无显著差异(P>0.05)。
2.3两组患者干预后的抑郁、焦虑和压力评分的平均值比较
表3显示了两组患者在干预后观察到DASS量表的评分存在显著差异(P<0.05),干预组的平均得分高于对照组。
3讨论
本研究旨在探讨护士主导的延续性护理干预措施,以电话随访(远程护理)的形式对血液透析患者抑郁、焦虑和压力的影响。由于像中国这样的发展中国家的慢性肾病患病率很高,本研究对这一人群进行了评估。根据本研究结果,两组患者在干预后DASS量表的评分存在显著差异(P<0.05),本研究发现接受延续性护理干预的观察组与只接受住院常规护理的对照组相比,观察组抑郁、焦虑和压力显著降低。有研究证实血液透析患者具有更高的抑郁和焦虑风险,换句话说就是焦虑和抑郁是血液透析患者常见的非精神病性精神障碍[14]。在其他一些研究报告中也证实了非药物干预在减少焦虑和抑郁方面的有效性,在一项随机对照研究中,3个月的认知行为疗法显著改善了抑郁症状评分[15]。另外一项关于运动训练的随机对照研究报告了有希望的结果[16]。Gitlin等人[17]得出结论,当对患有肾功能衰竭的抑郁症患者进行治疗时,心理培训是医生的一个适当选择。Sundsli等人[18]在一篇题为“自我保健电话谈话作为对75岁以上城市家庭生活者的健康促进干预”的文章中,总结出自我保健电话谈话显著改善了精神健康。Rollman等人[19]发现,电话随访与健康相关生活质量的临床显著改善相关。Kirsten等人[20]在题为“全膝关节置换术后护士的电话随访”的研究中,通过电话随访显示了与信息相关的护理以及通过电话随访与卫生专业人员的联系积极提高了患者满意度。
本研究结果显示与先前的研究结果一致,根据这些研究结果有必要评估有关电话随访的最佳科学证据,并获得有关使用手机的信息以及接受这些干预措施个人的临床和心理影响[21]。延续性护理作为一个新的领域,主要作为一种监测高风险患者接受侵入性手术的方式,使他们能够尽可能正常地过上正常生活。通过减少传统医院门诊监测的工作量,使医疗专业人员能够专注于实际需要住院治疗的患者的护理[22],这种护理策略被认为对患者服务更好,这也降低了患者再入院的风险,增强了他们的心理素质[23]。综上所述,本研究的结果有望为血液透析患者的有效随访提
供新的理论支持以改善他们的情绪和健康状况,本研究证实了临床专科护士通过延续性护理干预措施在改善血液透析患者心理健康方面的重要性。
参考文献
[1]Kimmel P L,Peterson R A.Depression in end-stage renal disease patients treated with hemodialysis:tools,correlates,outcomes,and needs[J].Seminars in dialysis,2005,18(2):91-97.
[2]Moser D K,Dracup K,Evangelista L S,et al.Comparison of prevalence of symptoms of depression,anxiety,and hostility in elderly patients with heart failure,myocardial infarction,and a coronary artery bypass graft[J].Heart&lung:the journal of critical care,2010,39(5):378-385.
[3]Chen W-L,Liu G-J,Yeh S-H,et al.Effect of back massage intervention on anxiety,comfort,and physiologic responses in patients with congestive heart failure[J].Journal of alternative and complementary medicine(New York,N.Y.),2013,19(5):464-470.
[4]Watnick S,Wang P-L,Demadura T,et al.Validation of 2 depression screening tools in dialysis patients[J].American journal of kidney diseases:the official journal of the National Kidney Foundation,2005,46(5):919-924.
[5]Hedayati S S,Grambow S C,Szczech L A,et al.Physician-diagnosed depression as a correlate of hospitalizations in patients receiving long-term hemodialysis[J].American journal of kidney diseases:the official journal of the National Kidney Foundation,2005,46(4):642-649.
[6]Rosengren A,Hawken S,Ôunpuu S,et al.Association of psychosocial risk factors with risk of acute myocardial infarction in 11 119 cases and 13 648 controls from 52 countries(the INTERHEART study):case-control study[J].The Lancet,2004,364(9438):953-962.
[7]Wassertheil-Soller S,Shumaker S,Ockene J.Depression and cardiovascular sequelae in postmenopausal women.The Women’s Health Initiative(WHI)[J].ACC Current Journal Review,2004,13(5):31-32.
[8]Bruce M L,Leaf P J.Psychiatric disorders and 15-month mortality in a community sample of older adults[J].American Journal of Public Health,1989,79(6):727-730.
[9]Kalender B,Ozdemir A C,Koroglu G.Association of depression with markers of nutrition and inflammation in chronic kidney disease and end-stage renal disease[J].Nephron.Clinical practice,2006,102(3-4):c115-21.
[10]Finkelstein F O,Wuerth D,Finkelstein S H.An approach to addressing depression in patients with chronic kidney disease[J].Blood purification,2010,29(2):121-124.
[11]Harris M,Richards K C.The physiological and psychological effects of slow-stroke back massage and hand massage on relaxation in older people[J].Journal of clinical nursing,2010,19(7-8):917-926.
[12]McGrath K C,Mondav R,Sintrajaya R,et al.Development of an environmental functional gene microarray for soil microbial communities[J].Applied and environmental microbiology,2010,76(21):7161-7170.
[13]Lovibond P F,Lovibond S H.The structure of negative emotional states:Comparison of the Depression Anxiety Stress Scales(DASS)with the Beck Depression and Anxiety Inventories[J].Behaviour Research and Therapy,1995,33(3):335-343.
[14]Duarte P S,Miyazaki M C,Blay S L,et al.Cognitive-behavioral group therapy is an effective treatment for major depression in hemodialysis patients[J].Kidney international,2009,76(4):414-421.
[15]Perales-Montilla C M,García-León A,Reyes-del Paso G A.Psychosocial predictors of the quality of life of chronic renal failure patients undergoing haemodialysis[J].Nefrologia:publicacion oficial de la Sociedad Espanola Nefrologia,2012,32(5):622-630.
[16]Ouzouni S,Kouidi E,Sioulis A,et al.Effects of intradialytic exercise training on health-related quality of life indices in haemodialysis patients[J].Clinical rehabilitation,2009,23(1):53-63.
[17]Gitlin M,Lee J A,Spiegel D M,et al.Outpatient red blood cell transfusion payments among patients on chronic dialysis[J].BMC nephrology,2012,13:145.
[18]Sundsli K,Söderhamn U,Espnes G A,et al.Self-care telephone talks as a health-promotion intervention in urban home-living persons 75+years of age:a randomized controlled study[J].Clinical interventions in aging,2014,9:95-103.
[19]Rollman B L,Belnap B H,LeMenager M S,et al.Telephone-delivered collaborative care for treating post-CABG depression:a randomized controlled trial[J].JAMA,2009,302(19):2095-2103.
[20]Szöts K,Konradsen H,Solgaard S,et al.Telephone follow-up by nurse following total knee arthroplasty-protocol for a randomized clinical trial(NCT 01771315)[J].BMC nursing,2014,13:14.
[21]Flanagan J.Postoperative telephone calls:timing is everything[J].AORN journal,2009,90(1):41-51.
[22]Mistiaen P,Poot E.Telephone follow-up,initiated by a hospital-based health professional,for postdischarge problems in patients discharged from hospital to home[J].The Cochrane database of systematic reviews,2006(4):CD004510.
[23]Thompson-Coon J,Abdul-Rahman A-K,Whear R,et al.Telephone consultations in place of face to face out-patient consultations for patients discharged from hospital following surgery:a systematic review[J].BMC health services research,2013,13:128.
关注SCI论文创作发表,寻求SCI论文修改润色、SCI论文代发表等服务支撑,请锁定SCI论文网! 文章出自SCI论文网转载请注明出处:https://www.lunwensci.com/yixuelunwen/20405.html