SCI论文(www.lunwensci.com):
摘要:苏醒期躁动是全麻术后常见并发症,发病机制及病因不明,严重影响患者预后。研究显示右美托咪定可提高全麻患者苏醒质量,减少成人苏醒期躁动的发生。本文就右美托咪定减少成人全麻术后苏醒期躁动的研究进展进行综述。
关键词:右美托咪定;全身麻醉;苏醒期躁动
本文引用格式:曹天宇,祝胜美,胡四平.右美托咪定减少成人全麻术后苏醒期躁动的研究进展[J].世界最新医学信息文摘,2019,19(63):74-75.
0引言
苏醒期躁动(Emergence Agitation,EA)是全麻术后早期出现的一种短暂的意识损害,患者苏醒但伴有精神状态的改变,表现为定向障碍、幻觉、意识混乱、烦躁不安及过度体动行为等[1]。EA因复杂多样的临床表现和严重的危害性受到人们的重视,但既往研究集中在儿童EA的病因学及流行病学的探索,对成人的研究报告很少[2-3]。右美托咪定是一种新型高选择性a2肾上腺素受体激动剂[4-5],可提高全麻患者的复苏质量,减少成人EA的发生[6-8],但机制不明,且暂无静脉应用右美托咪定防治成人全麻术后EA的指南推荐。鉴于此,本文就围术期静脉应用右美托咪定减少成人全麻术后EA的实际临床疗效、最佳给药策略及作用机制进行综述。
1EA病因及防治
全麻术后EA发病机制不明,成人发生率报告4.7%-22.2%不等[9-11],危险因素包括年龄、性别、认知障碍、术前焦虑、手术类型、吸入麻醉药、阿片类及苯二氮卓类药物、缺氧、快速觉醒、术后疼痛、导尿管及气管导管刺激等。EA多为自限性,但会延长恢复室滞留时间,可造成外伤、输液管路脱落,甚至手术切口裂开、出血、感染等,影响预后[2]。临床防治EA的主线是消除危险因素,如提供充足的术后镇痛,对消除明显危险因素情况仍未改善者,可应用快速短时的镇静药,如丙泊酚。右美托咪定作为一种新兴的麻醉辅助用药,有镇静、镇痛、神经保护等作用,可降低全麻术后成年患者EA发生率[4-8],目前在临床应用中脱颖而出。
2右美托咪定减少成人EA的探索
2.1临床疗效
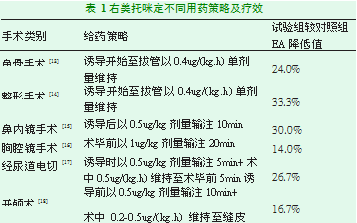
右美托咪定降低全麻术后EA的研究,既往集中在儿童身上,认为对儿童的效果是确切的[1]。近来大批学者在探索右美托咪定对成人全麻术后EA的作用(表1)。我国最新发布的《右美托咪定临床应用专家共识(2018)》[12],首次明确指出右美托咪定可以提高成人全麻术后复苏质量、减少EA的发生。
众多研究结果显示右美托咪定对减少成人全麻术后EA有一定临床意义[12-18],最新的专家共识首次指出右美托咪定这一功效,但是不同研究显示右美托咪定这一临床疗效差异显著。这些显著差异受EA发生的复杂性、潜在危险因素的不确定性所影响[11,19],同时目前对EA诊断缺乏统一的标准,尤其是成人,还有就是目前的研究样本量多偏小、各个研究方法也不相同,所以右美托咪定对降低成人全麻术后EA的真实有效性,即能在多大程度上减轻成人EA的发生,尚无定论。
2.2用药策略
欧洲麻醉学学会于2017年对右美托咪定的临床应用提出建议[20],2018年中国的麻醉学专家更新了《右美托咪定临床应用专家共识》[12],指出全身麻醉期间静脉应用右美托咪定三种给药方式:(1)麻醉诱导前给予负荷剂量或从麻醉诱导前至麻醉结束以一定剂量静脉持续泵注;(2)麻醉诱导后开始静脉持续泵注至麻醉结束前或结束后;(3)麻醉结束前开始静脉泵注至麻醉结束后。这三种给药策略涉及到负荷剂量、维持剂量及负荷剂量联合静脉维持三种用药方式,涉及诱导前、后给药及麻醉结束前给药三种给药时机,以及各种停药时间,所以右美托咪定的静脉用药策略非常复杂。大量研究显示右美托咪定各种给药策略防治成人全麻术后EA的有效性[12-18],但是多种给药策略孰优孰劣尚不清楚,目前也未见这方面的深入研究。欧洲麻醉学学会及中国麻醉学专家都提出了右美托咪定临床应用指导意见,但未涉及降低EA的最佳用药策略,目前无系统性评价以及指南推荐,所以右美托咪定在降低成人EA的最佳静脉用药方式、时机及剂量方面尚存争议,这需要诸位学者深入探讨,以期为右美托咪定防治EA的用药提供更加可靠的指导。
2.3防治机制
右美托咪定防治成人全麻术后EA机制不明。Anger等[21]认为,右美托咪定激动脑干蓝斑核a2肾上腺素受体产生的镇静、镇痛等作用,减轻术后疼痛、提高对伤害性刺激的耐受而减少EA的发生,此观点得到多位中国学者的认可[22]。Perez-Zoghbi等[23-24]研究显示,右美托咪定多种机制发挥的脑神经保护作用是减少EA发生的关键。还有夏勇军等[25]认为,术后急性痛觉过敏可促进EA的发生,而右美托咪定可降低苏醒期患者应激反应,防止中枢敏化、预防术后痛觉过敏发生。还有其他研究:右美托咪定减少EA危险因素的出现[26],如减轻炎症反应;右美托咪定提高中枢神经对缺氧的耐受,避免中枢神经缺氧而有脑保护作用[27];右美托咪定降低危险药物的用量,如阿片类药物[28];右美托咪定促进更为接近生理的睡眠-苏醒周期[29]。
目前右美托咪定降低成人全麻术后EA机制尚无定论,诸多见解有其合理性。一方面右美托咪定神经保护、稳定循环、促进生理性的睡眠周期等积极疗效,减少EA的发生;另一方面右美托咪定减少患者EA危险因素的暴露,如提高对不良刺激的耐受、减少阿片类药物应用。苏醒期躁动发病机制不明,这为我们研究右美托咪定减少EA发生形成了障碍,也许右美托咪定诸多作用正是某个节点上抑制了EA发病环节,我们不得而知。
3展望
随着医疗水平的提高,人们对全麻术后复苏质量提出更高要求。右美托咪定降低成人全麻术后EA疗效逐步得到证实,但具体机制不明,仍需更多的研究。在兼顾右美托咪定镇静、镇痛、抑制交感系统活性等作用的同时,我们需探讨右美托咪定降低成人全麻术后EA的最佳给药策略,以期让患者获取更大益处。
参考文献
[1]Vlajkovic GP,Sindjelic SR.Emergence delirium in children:many questions few answers[J].Anesth Analg,2007,104:84-91.
[2]Kwak KH.Emergence agitation/delirium:we still don't know[J].Korean journal of anesthesiology,2010,59(2):73-74.
[3]Munk L,Andersen LP.Emergence delirium[J].Perioper Pract,2013,23:251-4.
[4]Buck ML.Dexmedetomidine use in pediatric intensive care unit and procedural sedation[J].Pediatr Pharmacol Ther,2010,15(1):17-29.
[5]Weerink MAS,Struys MMRF,Hannivoort LN,et al.Clinical Pharmacokinetics and Pharmacodynamics of Dexmedetomidine[J].ClinPharmacokin et,2017,56(8):893-913.
[6]Djaiani G,Silverton N,Fedorko L,et al.Dexmedetomidine versus Propofol Sedation Reduces Delirium after Cardiac Surgery:A Randomized Controlled Trial[J].Anesthesiology,2016,124(2):362-368.
[7]Su X,Meng ZT,Wu XH,et al.Dexmedetomidine for prevention of delirium in elderly patients after non-cardiac surgery:a randomised,double-blind,placebo controlled trial[J].Lancet,2016,388(10054):1893-1902.
[8]Liu X,Xie G,Zhang K,et al.Dexmedetomidine vs propofol sedation reduces delirium in patients after cardiac surgery:A meta-analysis with trial sequential analysis of randomized controlled trials[J].Crit Care,2017,38:190-196.
[9]Xara D,Silva A,Mendonca J,et al.Inadequate emergence after anesthesia:emergence delirium and hypoactive emergence in the Post-anesthesia Care Unit[J].Clin Anesth,2013,25:439-46.
[10]Card E,Pandharipande P,Tomes C,et al.Emergence from general anaesthesia and evolution of delirium signs in the post-anaesthesia care unit[J].Br J Anaesth,2015,115:411-7.
[11]Kim HJ,Kim DK,Kim HY,et al.Risk factors of emergence agitation in adults undergoing general anesthesia for nasal surgery[J].Clin Exp Otorhinolaryng ol,2015,8(1):46-51.
[12]吴新民,薛张纲,马虹,等.右美托咪定临床应用专家共识(2018)[J].临床麻醉学杂志,2018,34(8):820-823.
[13]Kim DJ,Kim SH,So KY,et al.Effects of Dexmedetomidine on smooth emergence froom anesthesia in elderly patients undergoing orthopaedic surgery[J].Anesthesiology,2015,15(1):139.
[14]Fujisawa T,Komasawa N,Fujiwara A,et al.Effective dexmedetomidine administration for the prevention of emergence agitation and postoperative delirium in patients with a history of postoperative delirium[J].Masui,2015,65(4):395-397.
[15]Kwon SY,Joo JD,Cheon GY,et al.Effects of dexmedetomidine on the recovery profiles from general Anesthesia in patients undergoing endoscopic sinus surgery[J].Korean J Anesthesiol,2015,68(5):449-454.
[16]Lee SH,Lee CY,Lee JG,et al.Intraoperative Dexmedetomidine Improves the quality of recovery and postoperative pulmonary function in patients undergoing video-assisted thoracoscopic surgery[J].Medicine,2016,95(7):1-8.
[17]Kwon SY,Joo JD,Cheon GY,et al.Effects of dexmedetomidine infusion on the recovery profiles of patients undergoing transurethral resection[J].Korean Med Sci,2016,31(1):125-130.
[18]Song J,Ji Q,Sun,et al.TheOpioid-sparing effect of Intraoefative Dexmedetomidine infusion after craniotomy[J].Neurosurg Anesthesiol,2016,28(1):14-20.
[19]Mason KP,Jonathan H.Paediatric emergence delirium:a comprehensive review and interpretation of the literature[J].Br J Anaesth,2017,118(3):335-343.
[20]Jochen Hinkelbein,Massimo Lamperti.European Society of Anaesthesiology and European Board of Anaesthesiology guidelines for procedural sedation and analgesia in adults[J].Eur J Anaesthesiol,2017,34:1-19.
[21]Anger KE.Dexmedetomidine:a review of its use for the management Of pain,agitation,and delirium in the intensive care unit[J].Curr Pharm Des,2013,19(22):4003-4013.
[22]Chen W,Liu B,Zhang F,et al.Effect of dexmedetomidine on early postoperactive cognitive dysfunction and inflammatory factors in senile patients[J].Int J Clin Exp Med,2015,8(3):4601-4605.
[23]Perez-Zoghbi JF,Zhu W,Grafe MR,et al.Dexmedetomidine-mediated neuroprotection against sevoflurance-induced neurotoxicity extends to several brain regions in neonatal rats[J].Br J Anaesth,2017,119(3):506-516.
[24]Wang Y,Han R,Zuo Z.Dexmedetomidine post-treatment induces neuroprotection Via activation of extracellular signal-regulated kinase in rats with subarachnoid haemorrhage[J].Br J Anaesth,2016,116(3):384-392.
[25]夏勇军,李军鹏,李萌,等.右美托咪定联合地佐辛对老年高血压患者全麻苏醒期躁动及血流动力学影响[J].临床麻醉学杂志,2015,31(7):647-651.
[26]Maldonado JR,Wysong A,van der Starre PJ,et al.Dexmedetomidine and the reduction of postoperative delirium after cardiac surgery[J].Psychosomatics,2009,50(3):206-217.
[27]Seaman JS,Schillerstrom J,Carroll D,Brown TM.Impaired dxidative metabolismprecipitates delirium:a study of 101 ICU patients[J].Psychosomatics,2006,47(1):56-61.
[28]Pandharipande,Pratik,Shintani,et al.Lorazepam is an independent risk factor for transitioning to delirium in intensive care unit patients[J].Anesthesiology,2006,104(1):21-26.
[29]Nelson,Laura E,Lu,et al.The a 2-adrenoceptor agonist dexmedetomidine converges on an endogenous sleep-promoting pathway to exert its sedative effects[J].Anesthesiology,2003,98(2):428-43.
关注SCI论文创作发表,寻求SCI论文修改润色、SCI论文代发表等服务支撑,请锁定SCI论文网! 文章出自SCI论文网转载请注明出处:https://www.lunwensci.com/yixuelunwen/18470.html