SCI论文(www.lunwensci.com)
【摘要】 随着人口老龄化的加重,卒中、老年性肌少症患者均逐年增加,患者发病后的功能障碍、后续治疗越来越受到医务工作人 员的关注。卒中相关性肌少症这一概念的提出使人们对卒中后骨骼肌减少、功能改变等症状有了新的认识,但目前关于卒中相关性肌少症 的特别及其治疗的研究报道较少。本文从卒中相关性肌少症的特点、发病机制、不良后果、诊断及治疗管理等方面进行阐述。
【关键词】 卒中,肌少症,骨骼肌,吞咽困难,偏瘫,肌纤维
Stroke-associated sarcopenia research progress
LI Dongmei, ZHOU Muhua*
(Department of Geriatric Rehabilitation of Jiangbin Hospital of Guangxi Zhuang Autonomous Region,
Nanning 530021 Guangxi, China)
【Abstract】 With the aggravation of population aging, the stroke and senile sarcopenia patients are increasing year by year. The dysfunction and follow-up treatment of the associated patients have attracted more and more attention from medical staffs. The concept of stroke-related sarcopenia has led to a new understanding of skeletal muscle loss and functional changes after stroke. However, there are few reports on the special treatment of stroke-related sarcopenia. This article will illustrate the characteristics, pathogenesis, adverse consequences, diagnosis and treatment management of stroke-related sarcopenia.
【Keywords】 Stroke; Sarcopenia; Skeletal muscle; Dysphagia; Hemiplegia; Muscle fiber
1 引言
肌少症即肌肉减少症,最初由 Rosenberg 于 1997 年提出, 2019 年亚洲肌少症工作组(AWGS) 发布的肌少症诊断及治疗专家共识(AWGS2019) [1] 认为,肌肉力量和躯体功能下降均是肌肉质量下降 的结果,因此只要肌力或功能下降,合并肌肉质量 下降即可诊断为肌少症,若肌力和功能同时下降, 则为严重肌少症。近几年,人们提出了一些疾病相 关性肌少症的概念,卒中相关性肌少症则是其中之 一 [2] ,表明卒中与肌少症的发生密不可分,应区别 于老年性肌少症 [3]。
2 卒中相关性肌少症与衰老过程中肌少症的区别
2.1 患病率较高 根据最近的一项系统回顾和荟 萃分析 [4] ,卒中相关性肌少症的发病率约 42%,其 中男性(45%) 高于女性(39%) ;而心血管疾病、 糖尿病和呼吸系统疾病导致的继发性肌少症发生率分别为 31.4%,31.1%、26.8%; 而健康老年人肌少 症发病率仅有 0~15%[5]。
2.2 与年龄无关 卒中发生后偏瘫侧肢体肌肉单 元迅速减少,在卒中发生后 4 h 可观察到肌肉组织 结构适应性变化,这可能与支配肌肉的运动神经 元突触传递中断有关 [6] ;在卒中发生 1 周内,未受 影响的健侧肢体也会出现肌肉无力 [7] ,患侧肢体肌 萎缩更明显。而衰老过程中的肌肉减少则是年龄 相关的渐进性肢体肌肉减少,两侧肢体肌萎缩程度 相近。
2.3 骨骼肌结构的变化 正常情况下,在衰老过 程中,肌肉纤维从快收缩肌球蛋白重链(myosin heavy chain,MHC) 转换为富含线粒体的慢收缩 (MHC I 型)肌肉纤维;而卒中相关性肌少症的一 个特殊特征是慢肌纤维向快肌纤维转变 [8]。
3 卒中相关性肌少症的发病机制
卒中相关性肌少症与老年性肌少症具有相同的 发病机制:如运动减少所致萎缩、神经 - 肌肉功能 减弱、激素变化(胰岛素、雌激素、雄激素、生长 激素及糖皮质激素等)、促炎性细胞因子水平增高、 肌细胞凋亡、营养不良,以下为影响卒中相关性肌少症发病的特发因素 [8]。
3.1 肌肉失神经支配及纤维表型改变 卒中可引 起局部脑神经功能缺失,致使肌肉单元的去神经 支配及神经再支配,导致依赖于无氧代谢的快收 缩 MHC II 型肌肉纤维增加 [9]。在患侧下肢中快速 MHC II 型肌肉纤维的比例与步态缺陷的严重程度 呈负相关 [10]。
3.2 全身分解代谢增强 卒中后大脑局部神经损 伤、自主神经系统失衡导致全身炎症反应,合成 代谢减少、分解代谢信号增加也是卒中后肌肉减 少加速的重要原因 [8]。卒中后偏瘫侧肌生长抑制素 的 mRNA 表达水平较非偏瘫侧高 40%,抗阻训练 后偏瘫侧中肌肉生长抑制素 mRNA 表达水平下降 49%,非麻痹肌中肌肉生长抑制素 mRNA 表达水平 下降 27%,表明肌生长抑制素在偏瘫后肌萎缩中 可能存在重要的调控作用 [11]。而肿瘤坏死因子 -α mRNA 水平在偏瘫侧肢体中是健康人下肢肌肉的2.8 倍,较非偏瘫侧肢体高 1.6 倍 [12]。且因全身分 解代谢被激活,胰岛素抵抗造成脂质沉积,蛋白质 分解,肌肉中脂肪含量增加,肌肉含量减少 [13-15]。
3.3 其他 有研究发现,卒中患者入院时的血红 蛋白水平低与肌肉减少、体力功能恢复较差和吞咽 困难有关 [16-18] ;肌少症可能导致急性卒中后患者的 口咽肌肉质量和力量损失, 从而导致口腔肌肉减少, 进而造成口腔功能障碍及营养不良,加重肌少症。
4 卒中相关性肌少症造成的不良后果
根据世界卫生组织统计数据显示,脑血管意外 是全球第 2 大死亡原因和第 3 大残疾原因,且卒中 相关性肌少症患者预后更差。
4.1 运动能力下降 Abe[19] 研究发现,缺血性卒中 患者发病时的低骨骼肌质量是急性期出院时步行功 能的独立预测因子,轻、中度卒中患者在低骨骼 肌质量指数(SMI)时存在明显的行走困难。一项 纳入 164 例老年急性缺血性卒中患者的研究 [20] 通 过生物电阻分析发现,62%(101 例)的患者存在 SMI 定义的骨骼肌质量缺陷,且年龄越高,骨骼肌 质量缺陷比例越高。与无骨骼肌质量缺陷的患者比 较,骨骼肌质量缺陷比例越高的患者住院时间越长, 且治疗后改良 Rankin 评分明显更低 [21]。
4.2 日常生活能力下降 Matsushita等[22] 研究认为,卒中相关肌减少症是男性患者康复后日常生活活动 能力的一个预测指标,肌少症患者在出院时的功能 独立量表运动得分更低,但对女性不适用。
4.3 肺功能下降 有研究显示,50 岁以上脑卒中 患者握力、肺功能、最大吸气压力及最大呼气压力, 较一般老年人降低,握力与肺功能和最大呼气压力 相关 [23]。
4.4 认知功能下降 陈长等 [24] 评估老年轻型急性 缺血性脑卒中患者的认知功能发现,肌少症组简易 智能量表总分、定向力、记忆、注意力和计算力、 语言能力均下降,且回归分析显示,在首次发病的 老年轻型急性缺血性卒中患者中,肌少症是发生卒 中后认知障碍的独立危险因素。
5 卒中相关性肌少症的诊断
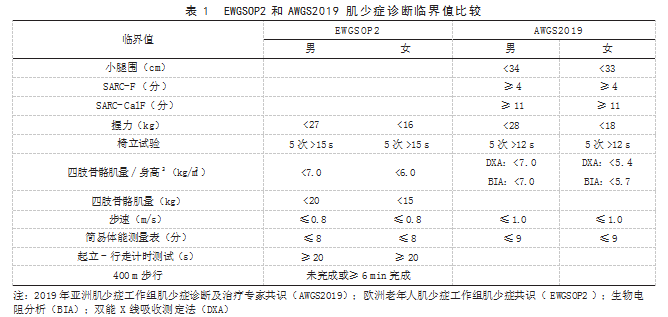
根据近年来相关的研究数据,卒中相关性肌少 症患病率在 16.8%~60.3%[4]。目前临床诊断肌少症一 般采用 AWGS2019[1] 和欧洲老年人肌少症工作组 2018 年发布的欧洲肌少症共识(EWGSOP2)[25]。这两个诊 断标准推荐使用小腿围问卷、SARC-F量表 [ 肌肉力量 S(Strength)、辅助行走 A(Assistancein walking)、 起立 R(Risefrom achair)、爬楼梯 C(Climb stairs)- 跌倒 F(Falls) ] 或 SARC-F 量表联合小腿围问卷 筛查肌少症;然后使用双能 X 线吸收测定法和生物 电阻分析法评估四肢骨骼肌量,使用握力和(或) 椅立试验评估肌力;最后进行体能评价,应用简易 体能测量表、5 次起坐时间 / 起立 - 行走计时测试 和 6 m/400 m 步行测试评估肌少症的严重程度。两 个诊断标准临界值区别见表 1.但卒中患者发病前 的肌肉状况也会对研究结果产生一定的混淆,而卒 中前肌肉萎缩对卒中的不良预后及严重程度有预测 价值 [26-28]。大部分卒中后肌少症的研究受肌少症的 诊断标准和方法限制,纳入的研究对象身体机能相 对较好,然而现实中卒中后不能完成起坐试验或步 行试验患者较多,以步态速度或简易体能测量表等 评估方法来定义肌少症不适合全部卒中患者。目前 还有通过活检、 CT、 磁共振成像或磁共振波谱分析 检查测定大腿中部或全身肌肉质量评估、腰椎水平 CT 图像、CT 腰肌测量、CT 颞肌测量、超声评估 胫前肌厚度、肌酸稀释试验及其他特定的生物标志 物(如尿肌联素)等评估手段 [25.29-32]。
6 卒中相关性肌少症的治疗与管理
2021 年中国老年人肌少症诊疗专家共识推荐, 肌少症患者在营养补充的基础上进行抗阻训练,并 联合有氧、拉伸和平衡运动以改善躯体功能 [33]。而 针对卒中后肌少症的治疗及管理目前尚未有明确的 指南或共识,主要治疗方法与老年性肌少症大致 相同,除运动及营养干预之外,药物治疗包括维 生素 D、选择性雄激素受体调节剂、乳清蛋白等, 但目前药物治疗对肌少症患者的疗效无法确定 [25]。 Ogawa等[34] 对 159例卒中患者进行研究, 发现>80岁 的卒中后肌少症患者经过康复治疗后SMI显著升高。 此外, 住院时间和蛋白质摄入量与SMI 的增加相关。 Ohyama 等 [20] 研究表明,骨骼肌质量缺陷患者的体 质量指数与白蛋白水平降低相关。Yoshihiro 等 [16] 的研究则发现,卒中后接受康复治疗的患者入院时 的低血红蛋白水平与肌肉减少、体力恢复较差和吞 咽困难有关。而通过提高人体白蛋白、血红蛋白含 量是否能改善卒中相关性肌少症尚未证实 [35]。有研 究发现 [36] ,在急性卒中患者中,与仅使用 3 d 依达 拉奉治疗比较,使用 10~14 d 的患者患侧腿部肌肉 萎缩的发生较卒中 3 个月后显著减少。因此,除了 运动及营养干预外,尚有其他适合治疗及管理卒中 相关性肌少症的方法。
7 小结
当前人们已认识到卒中相关性肌少症与老年性 肌少症的患病率、发病机制、不良后果不同。在诊治卒中患者时应注意加强对卒中相关性肌少症的识 别和诊断,及时筛查评估,并通过运动锻炼、营养 支持及药物治疗等措施干预,降低卒中相关性肌少 症患者的致残率。
参考文献
[1] Chen LK,Woo J,Assantachai P,et al. Asian Working Group for Sarcopenia:2019 consensus update on sarcopenia diagnosis and treatment[J]. J Am Med Dir Assoc,2020.21(3): 300-307.
[2] Nadja S,Doehner W. Sarcopenia in stroke-facts and numbers on muscle loss accounting for disability after stroke[J]. J Cachexia Sarcopenia Muscle,2011.2( 1): 5-8.
[3] 王亚楠, 吴思缈, 刘鸣 . 中国脑卒中 15 年变化趋势和特点 [J]. 华西医学,2021.36(6):803-807.
[4] Ya S ,Michiko Y ,Mika O. Prevalence of stroke-related sarcopenia: A systematic review and meta-analysis[J]. J Stroke Cerebrovasc Dis,2020.29(9): 105092.
[5] Reijnierse EM,Trappenburg MC,Leter MJ,et al. The impact of different diagnostic criteria on the prevalence of sarcopenia in healthy elderly participants and geriatric outpatients[J]. Gerontology,2015.61(6): 491-496.
[6] Arasaki K ,Igarashi O ,Ichikawa Y ,et al. Reduction in the motor unit number estimate(MUNE)after cerebral infarction[J]. J Neurol Sci,2006.250( 1/2): 27-32.
[7] Harris ML ,Polkey MI ,Bath PM ,et al. Quadriceps muscle weakness following acute hemiplegic stroke[J]. Clin Rehabil, 2001.15:274-281.
[8] Scherbakov N,Haehling S,Anker SD,et al. Stroke induced Sarcopenia:Muscle wasting and disability after stroke[J]. Int J Cardiol,2013.170(2): 89-94.
[9] Papadatou MC. Sarcopenia in hemiplegia[J]. J Frailty Sarcopenia Falls,2020.5(2): 38-41.[10] Deyne PG,Hafer-Macko CE,Ivey FM,et al. Muscle molecular phenotype after stroke is associated with gait speed[J]. Muscle Nerve,2004.30(2): 209-215.
[11] Ryan AS,Ivey FM,Serra MC,et al. Sarcopenia and physical function in middle-aged and older stroke survivors[J]. Arch Phys Med Rehabil,2017.98(3): 495-499.
[12] Hafer-Macko CE ,Yu S ,Ryan AS ,et al. Elevated tumor necrosis factor- alpha in skeletal muscle after stroke[J]. Stroke, 2005.36(9): 2021-2023.
[13] Ryan AS,Dobrovolny CL,Smith GV,et al. Hemiparetic muscle atrophy and increased intramuscular fat in stroke patients[J]. Arch Phys Med Rehabil,2002.83( 12): 1703-1707.
[14] Matsushita T,Nishioka S,Taguchi S,et al. Sarcopenic obesity and activities of daily living in stroke rehabilitation patients:A cross- sectional study[J]. Healthcare(Basel),2020.8(3): 255.
[15] English C,Thoirs K,Coates A,et al. Changes in fat mass in stroke survivors:A systematic review[J]. Int J Stroke,2012.7 (6): 491-498.
[16] Yoshimura Y,Wakabayashi H,Nagano F,et al. Low hemoglobin levels are associated with sarcopenia,dysphagia,and adverse rehabilitation outcomes after stroke[J]. J Stroke Cerebrovasc Dis, 2020.29( 12): 105405.
[17] Shiraishi A,Yoshimura Y,Wakabayashi H,et al. Prevalence of stroke-related sarcopenia and its association with poor oral status in post-acute stroke patients:Implications for oralsarcopenia[J]. Clin Nutr,2018.37( 1): 204-207.
[18] Yoshimura Y ,Wakabayashi H ,Bise T ,et al. Prevalence of sarcopenia and its association with activities of daily living and dysphagia in convalescent rehabilitation ward inpatients[J]. Clin Nutr,2018.37(6 Pt A): 2022-2028.
[19] Abe T ,Iwata K ,Yoshimura Y ,et al. Low muscle mass is associated with walking function in patients with acute ischemic stroke[J]. J Stroke Cerebrovasc Dis,2020.29( 11): 105259.
[20] Ohyama K,Watanabe M,Nosaki Y,et al. Correlation between skeletal muscle mass deficit and poor functional outcome inpatients with acute ischemic stroke[J]. J Stroke Cerebrovasc Dis,2020.29 (4): 104623.
[21] Jang Y ,Im S ,Han Y ,et al. Can initial sarcopenia affect poststroke rehabilitation outcome?[J]. J Clin Neurosci,2020.71: 113-118.
[22] Matsushita T ,Nishioka S ,Taguchi S,et al. Sarcopenia as a predictor of activities of daily living capability in stroke patients undergoing rehabilitation[J]. Geriatr Gerontol Int,2019.19( 11): 1124-1128.
[23] Kim NS. Correlation between grip strength and pulmonary function and respiratory muscle strength in stroke patients over 50 years of age[J]. J Exerc Rehabil,2018.14(6): 1017-1023.
[24] 陈长,刘辉,蔺阳刚,等 . 首次发病的老年轻型急性缺血性卒中患者肌少症与卒中后认知障碍相关性研究 [J]. 中华老年医学杂志, 2021.40(4):444-449.
[25] Cruz-Jentoft AJ,Bahat G,Bauer J,et al. Sarcopenia:Revised European consensus on definition and diagnosis[J]. Age Ageing,2019.48( 1): 16-31.
[26] Nozoe M,Kanai M,Kubo H,et al. Prestroke sarcopenia and stroke severity in elderly patients with acute stroke[J]. J Stroke Cerebrovasc Dis,2019.28(8): 2228-2231.
[27] Nozoe M,Kubo H,Kanai M,et al. Sarcopenia risk and diabetes mellitus are independent factors for lower limb muscle strength in older patients with acute stroke:A cross-sectional study[J].Nutrition,2021.84:111025.
[28] Nozoe M,Kanai M,Kubo H,et al. Prestroke sarcopenia and functional outcomes in elderly patients who have had an acute stroke:A prospective cohort study[J]. Nutrition ,2019 ,66:44-47.
[29] Jung HJ ,Lee YM ,Kim M ,et al. Suggested assessments for sarcopenia in patients with stroke who can walk independently[J].Ann Rehabil Med,2020.44( 1): 20-37.
[30] 齐萌,张思伟,刘波 . 肌少症的 CT、MR 诊断及临床意义 [J].中国骨质疏松杂志, 2018.24(11):1530-1534.
[31] Nakanishi N,Tsutsumi R,Hara K,et al. Urinary titin is a novel biomarker for muscle atrophy in nonsurgical critically ill patients:A two-center,prospective observational study[J]. Crit Care Med,2020.48:1327-1333.
[32] Nakanishi N ,Okura K ,Okamura M ,et al. Measuring and monitoring skeletal muscle mass after stroke:A review of current methods and clinical applications[J]. J Stroke Cerebrovasc Dis,2021.30(6): 105736.
[33] 刘娟,丁清清,周白瑜,等 . 中国老年人肌少症诊疗专家共识(2021) [J]. 中华老年医学杂志, 2021.40(8) :943-952.
[34] Ogawa T ,Suenaga M. Elderly patients after stroke increase skeletal muscle mass by exercise therapy in rehabilitation wards[J].J Stroke Cerebrovasc Dis,2021.30(9): 105958.
[35] Yoshimura Y,Bise T,Shimazu S,et al. Effects of a leucine- enriched amino acid supplement on muscle mass,muscle strength, and physical function in post-stroke patients with sarcopenia:A randomized controlled trial[J]. Nutrition,2019.58:1-6.
[36] Naritomi H,Moriwaki H,Metoki N,et al. Effects of edaravone on muscle atrophy and locomotor function inpatients with ischemic stroke:A randomized controlled pilot study[J]. Drugs R D,2010.10(3): 155-163.
关注SCI论文创作发表,寻求SCI论文修改润色、SCI论文代发表等服务支撑,请锁定SCI论文网!
文章出自SCI论文网转载请注明出处:https://www.lunwensci.com/yixuelunwen/72162.html