SCI论文(www.lunwensci.com):
摘要:目的 评估急性生理与慢性健康状况评分( APACHE Ⅱ)预测产科 ICU 患者病情危重程度及预后的价值。 方法 收集 2019 年 8 月至 2020 年 8 月入住四川大学华西第二医院 ICU 超过 24 h 的孕产妇相关数据进行回顾性分析, 采用受试者操作曲线( ROC )曲线下面积 ( AUC )评估 APACHE Ⅱ评分预测产科危重症的能力。 结果 研究期间共有 19 438 名孕产妇入院分娩, 378 例入住 ICU,研究纳入 352 例, 290 例发生产科危重症, 发生率为 14.92/1 000;死亡 2 例, 死亡率为 1.03/10 000。产科 ICU 患者 APACHE Ⅱ评分总体偏低, 总体中位数为 4 ( 2, 6 ), 危重症组高于非危重症组( P<0.001 )。随着 APACHE Ⅱ评分的增加, 患者 ICU 住院时间延长( P<0.001 ), 使用呼吸机、持续 肾脏替代治疗( CRRT )、体外膜肺氧合( ECMO )的比例增加( P<0.05 )。 APACHE Ⅱ评分的 AUROC 为 0.697 ( 95% CI, 0.629~0.764 ), 当截断值为 10 分时, 预测产科危重症的敏感度为 10.34% ( 95% CI, 7%~14% ) , 特异度为 98.39% ( 95% CI, 91%~100% ) , 阳性预测值 ( PPV )为 96.77% ( 95% CI, 83%~100% ) , 阴性预测值( NPV )为 8.08% ( 95% CI, 15%~24% ); 预测患者死亡率为 8.43% ( 95% CI, 8.77%~25.89% )。 结论 APACHE Ⅱ评分在一定程度上能评估产科患者疾病严重程度,但预测产科危重症的敏感度低,且易高估患者死 亡率,不适用于预测产科危重症的发生。
关键词: APACHE Ⅱ评分 ; 孕产妇死亡 ; 产科危重症
Application value of Acute Physiology and Chronic Health Evaluation Ⅱ score in critical ill patients admitted to obstetric ICU
XU Yonghui1,2, XIAO Fei1,2*
[1. Department of Obstetrics and Gynecology, West China Second Hospital, Sichuan University;2 Key Laboratory of Birth Defects and Related Diseases of Women and Children, West China Second Hospital, Sichuan University, Ministry of Education ,Chengdu, Sichuan 610041, China ]
Abstract: Objective To evaluate the ability of Acute Physiology and Chronic Health Evaluation Ⅱ (APACHE Ⅱ) in predicting the severity and prognosis of critically ill patients in obstetric ICU of West China Second University Hospital. Methods Related data of pregnant women admitted to ICU for more than 24 hours from August 2019 to August 2020 were retrospectively analyzed, and area under curve (AUC) was used to evaluate the ability of APACHE Ⅱ score to predict critical illness. Results During the study period, a total of 19 438 pregnant women were hospitalized for delivery, 378 were admitted to ICU, and 352 were included in the study. A total of 290 women developed obstetric critical illness, with an incidence of 14.92/1 000. Two patients died, the mortality rate was 1 .03/10 000. The APACHE Ⅱ score of obstetric ICU patients was generally low, with a median of 4(2, 6), and the critical group was higher than the non-critical group (P<0.001) The length of ICU stay increased with the increase of APACHE Ⅱ score (P<0.001), as well as the proportion of using ventilator, continuous renal replacement therapy(CRRT)、extracorporeal membrane ox ygenation(ECMO)(P<0.05). The AUC of APACHE Ⅱ score for predicting obstetric critical care was 0.697 (95%CI, 0.629~0.764). When the cut-off value was 10, the sensitivity was 10.34% (95%CI, 7%~14%), 98.39% (95% CI, 91%~100%), positive predictive value (PPV) of 96.77% (95% CI, 83%~100%), negative predictive value (NPV) of 8.08% (95% CI, 15%~24%), and the predicted mortality rate was 8.43% (95%CI,8.77%~25.89%). Conclusion APACHE Ⅱ score can evaluate the severity of disease in obstetric patients to a certain extent, but it is not suitable for predicting the occurrence of obstetric critical illness due to its low sensitivity and easy overestimate of mortality rate.
Keywords: APACHE Ⅱ score; Maternal mortality; Obstetric critical care; Intensive care unit
控制孕产妇死亡率仍是全球卫生保健系统的一个主要 问题,在不同国家存在巨大差异,发展中国家明显高于发 达国家 [1] 。产科严重并发症是产妇死亡的主要原因 [2] 。因 此,孕产妇安全监测不仅应关注孕产妇死亡率,还应关注 孕产妇严重并发症的发病率。有效早期识别产科危重症有 助于提高孕产妇安全 [3] 。APACHE Ⅱ评分是一种预测患者 病情程度及预后的评分系统,在综合 ICU、急诊等已应用 广泛 [4], 但在产科患者中的应用效果存在争议 [5-6]。本研究 的主要目的是通过 ROC 曲线下面积、敏感度、特异度等验 证 APACHE Ⅱ评分预测孕产妇危重症的有效性。
1 资料与方法
1.1 一般资料 2019 年 8 月至 2020 年 8 月共有 19 438 名产妇在四川大学华西第二医院分娩,ICU 收治 378 名, 对所有分娩 42 天内的孕产妇,入 ICU 住院超过 24 h 的患 者进行回顾性研究。
1.2 方法 纳入标准:ICU 住院时间大于 24 h 的产科患 者,对其 APACHE Ⅱ评分进行核查。排除标准:ICU 住院 时间小于 24 h 的患者。研究终点:产科危重并发症,包 括以下情况:①高血压使用静脉降压药治疗、HELLP 综合 征、子痫 [7] ;②妊娠合并心脏病患者,采用改良版世界 卫生组织孕产妇心血管风险分类法(mWHO)评估妊娠风 险,mWHO 风险分级为Ⅲ级以上 [8] ;③严重产后出血,估 计出血≥2 000 mL, 输红细胞悬液≥3 U 或行子宫切除 术或行子宫动脉栓塞术 [9] ;④其他:脓毒症、各种类型 的休克、肺水肿、深静脉血栓形成、酮症酸中毒、颅内 肿瘤、癫痫持续状态、急性胰腺炎、肝衰竭、急性脂肪 肝等 [10– 13]。观察患者 ICU 住院时间、年龄、孕周等指标。 将住院期间发生产科严重并发症者归为危重症组,未发生 严重并发症者为非危重症组。本研究经四川大学华西第二 医院医学伦理委员会审批通过。
1.3 统计学方法 将结果制成表格,SPSS 25.0 版本进行 统计分析,所有定量资料采用 Shapiro-Wilk 检验进行数 据正态性检验,若服从正态分布,则用“均数 ± 标准 差”表示, 并采用独立样本 t 检验比较; 若偏态分布则采 用中位数和四分位数 [M( P25,P75 )] 表示,组间比较采 用 Mann-Whitney U 检验。定性资料用率表示,组间比较 采用 χ2 检验或 Fisher 确切概率法。ROC 曲线下面积用于确 定预测危重症的发生,计算敏感度、特异度、阳性预测值(PPV)、阴性预测值(NPV)。对于所有的统计检验, P<0.05 为有统计学意义。
2 结果
2.1 临床特征 研究期间共有 19 438 名孕产妇入院分 娩,ICU 收治共 378 名,ICU 入住率 19 .45/1 000,352 例 患者纳入研究。290 例患者出现严重并发症,发生率为14.92/1 000,其中 2 例死亡,死亡率 1.03/10 000。其中 1 例死于肺栓塞, 1 例死于重度肺动脉高压。收治 ICU 最 常见的原因依次是高血压疾病,心血管疾病、产科出血、感染、急性肺水肿、肺栓塞,见表 1。
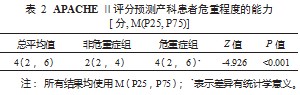
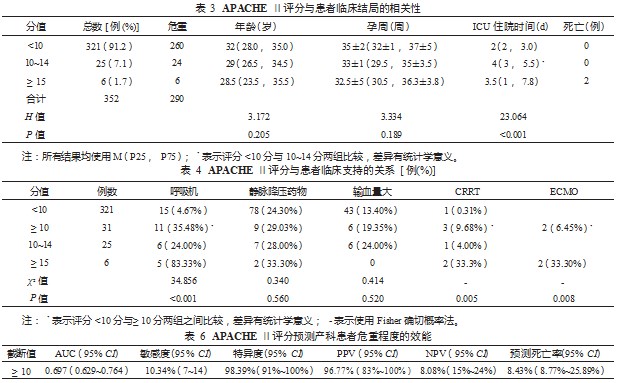
2.2 APACHE Ⅱ与产科患者病情严重程度的关系 结果 显示,APACHE Ⅱ评分 4 分(2 分,6 分),危重症组高于 非危重症组,两者相比差异有统计学意义(P<0.001 ), 见表 2。随着 APACHE Ⅱ评分的增加,患者年龄与孕周有 减小的趋势,但结果差异没有统计学意义,而 ICU 住院 时间随着 APACHE Ⅱ评分的增加而延长,在 APACHE Ⅱ评分≥10 分的患者与 <10 分患者相比,结果差异有 统计学意义(P<0.001 )。APACHE Ⅱ评分≥15 分时,死 亡风险增加,见表 3。然而,在评分 <10 分的 321 例 ( 91 .2%)患者中,有 260 例发生了产科危重症。结果提 示,APACHE Ⅱ评分与产科患者病情严重程度有一定的关系,但总体上不能较好地反映产科危重症的发生。
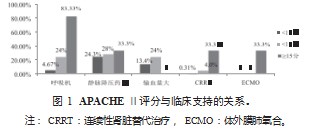
研究发现, APACHE Ⅱ评分≥10 分的患者, 35.48% 使用呼吸机支持, 29.03% 使用静脉降压药物, 19.35% 输 血量大(即住院期间输注红细胞悬液 >3 U,输注新鲜冰 冻血浆 >400 mL,输注辐照单采血小板 >2 个治疗量,满 足上述 3 条至少 1 条), 3% 行 CRRT, 6.45% 行 ECMO 治疗;与 APACHE Ⅱ评分 <10 分的患者比较,呼吸机、 CRRT 及 ECMO 支持的 比例差异均 有统计学 意义(均 P<0.05) ,使用静脉降压药物及输血量大的比例增加, 但差异无统计学意义。评分≥15 分时,除输血量以外, 上述临床支持比例均明显增加(表 4、图 1 ) 。结果表 明, APACHE Ⅱ评分能在一定程度上反映患者的病情严重 程度。
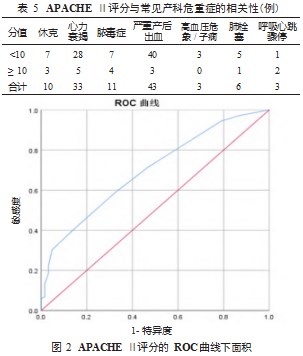
2.3 APACHE Ⅱ评分预测产科危重症的效能评价 实 验进一步分析了 APACHE Ⅱ评分与部分常见产科危重 症的相关性,结果提示,大部分发生危重并发症的患者 APACHE Ⅱ评分 <10 分(表 5 ),APACHE Ⅱ评分预测产 科危重症的效能较低。进一步研究发现,APACHE Ⅱ评分预测危重孕产妇的特异度及 PPV 高,但敏感度及 NPV 较 低,且死亡率预测值高于实际死亡率,见表 6、图 2。
3 讨论
降低孕产妇死率仍是卫生健康系统面临的严峻挑 战 [7] ,通过预测产科危重症并及时给予干预措施是降低死亡风险的重要举措。APACHE Ⅱ评分在评估非产科患者 病情严重程度、预估患者死亡率中有较高的应用价值,但 在产科患者人群的研究相对较少,目前有部分学者提出 APACHE Ⅱ评分不适用于产科人群 [14- 15]。为此, 本研究主 要目的在于评估 APACHE Ⅱ评分在专科医院产科 ICU 患 者中预测产科危重症及预后的临床价值。
产科患者入 ICU 最常见原因依次是高血压、心血管疾 病、产科出血和感染等。危重症患者 APACHE Ⅱ评分高 于非危重症组, 但 APACHE Ⅱ评分总体较低, 大部分患者 APACHE Ⅱ评分低于 10 分,该结果与部分研究 [5, 16] 结果 不一致,分析其原因考虑以下两点:①目前全球医疗水平 不均衡,孕产妇死亡率在各个国家地区之间差异较大,疾 病危重程度有差异; ②每个研究机构 ICU 入院的指征不一 致, 综合医院 ICU 的产科患者病情危重程度可能重于专科 医院产科 ICU。
随着 APACHE Ⅱ评分增加,ICU 住院时间随之延长,患 者年龄、孕周差异无统计学意义。当评分≥10 分时,无创或 有创呼吸机、 CRRT、ECMO 支持的比例增加(P<0.05 ), 高血压患者使用静脉降压药物降压的比例、输血量随之增 加, 15 分以上时死亡风险明显增加。但是, APACHE Ⅱ评 分 <10 分的患者中仍有部分发生休克、心力衰竭、严重产后 出血、脓毒症、肺栓塞、高血压危象或子痫、呼吸心跳骤停 等严重并发症。其中, 4.3% 的患者使用呼吸机支持, 23% 高血压患者使用静脉降压药物控制血压, 13.08% 的患者输 血量大。APACHE Ⅱ评分能在一定程度上反映产科患者病 情危重程度,但不能完全准确预测其产科危重症的发生。
与 XI, MUENCH 等 [6,17] 研究结果类似, APACHE Ⅱ评 分预测产科危重症的能力偏低, 其 AUC 为 0.697, 特异度 及 PPV 高,但敏感度及 NPV 均较低。其次, APACHE Ⅱ评 分易高估产科患者死亡率,本研究中其预测孕产妇死亡率 为 8.43%, 而实际死亡率为 1.03/10 000, 结果与 KARNAD 和刘慧姝等 [15, 18] 研究一致。
本研究的局限性在于,该研究为单中心回顾性分析, 样本量相对较少,结论仍需要更多的研究进一步验证。
4 结论
APACHE Ⅱ评分能从一定程度上反映产科患者疾病严 重程度,但是该评分预测产科危重症的敏感度较低,且易 高估孕产妇死亡率, 不适用于预测产科危重症的发生。尚需 进行更多的研究建立一项新的适用于预测所有产科危重症 及预后的评分系统,为降低孕产妇死率提供更高的保障。
参考文献
[1] DZAKPASU S, DEB-RINKER P, ARBOUR L, et al. Severe maternal morbidity surveillance: Monitoring pregnant women at high risk for prolonged hospitalisation and death[J]. Paediatric and Perinatal Epidemiology, 2020, 34(4): 427-439.
[2] SCHAAP T, BLOEMENKAMP K, DENEUX-THARAUX C, et al.Defining definitions: a Delphi study to develop a core outcome set for conditions of severe maternal morbidity[J]. BJOG : An International Journal of Obstetrics and Gynaecology, 2019, 126(3): 394-401.
[3] MHYRE J M, D' ORIA R, HAMEED A B, et al. The maternal early warning criteria: a proposal from the national partnership for maternal safety[J]. Obstetrics and gynecology, 2014, 124(4): 782-786.
[4] KADZIOLKA I, ŚWISTEK R, BOROWSKA K, et al. Validation of APACHE Ⅱ and SAPS Ⅱ scales at the intensive care unit along with assessment of SOFA scale at the admission as an isolated risk of death predictor[J]. Anaesthesiology Intensive Therapy, 2019, 51(2): 107-111.
[5] KRISHNA KUMAR M, JOSHI A, SARASWAT M, et al. Near-Miss incidents in obstetric patients admitted to an intensive care unit of a tertiary care center in eastern india: A retrospective cohort study[J]. Journal of Obstetrics and Gynecology of India, 2021(0123456789).
[6] XI J, REN H, ZHANG H, et al. Clinical characteristics of critically ill pregnant women with different admission methods to intensive care unit: Data analysis from 2006 to 2019 in the university hospital[J]. Chinese Critical Care Medicine, 2021, 33(10): 1249- 1254.
[7] SINKEY R G, BATTARBEE A N, BELLO N A, et al. Prevention,diagnosis, and management of hypertensive disorders of pregnancy: a comparison of international guidelines[J]. Current Hypertension Reports, 2020, 22(9): 66.
[8] REGITZ-ZAGROSEK V, ROOS-HESSELINK J W, BAUERSACHSJ, et al. 2018 ESC Guidelines for the management of cardiovascular diseases during pregnancy[J]. Kardiologia Polska, 2019, 77(3): 245-326.
[9] CLINICAL GUIDELINES - QUEENSLAND HEALTH Q .Maternity and Neonatal Clinical Guideline[J]. (2017- 12-01)[2021- 07 - 01] . https://www.health . qld .gov. au/ __data/assets/pdf_ file/0015/140136/g-pph.pdf
[10] VASQUEZ D N, DAS NEVES A V, VIDAL L, et al. Characteristics, outcomes, and predictability of critically ill obstetric patients: A multicenter prospective cohort study[J]. Critical Care Medicine, 2015, 43(9): 1887- 1897.
[11] LIM E, MOUYIS M, MACKILLOP L . Liver diseases in pregnancy[J]. Clinical Medicine, 2021, 21(5): 441-445.
[12] SEGEV L, SEGEV Y, RAYMAN S, et al. Acute appendicitis during pregnancy: Different from the nonpregnant state?[J]. World Journal Of Surgery, 2017, 41(1): 75-81.
[13] CRUCIAT G, NEMETI G, GOIDESCU I, et al. Hypertriglyceridemia triggered acute pancreatitis in pregnancy - diagnostic approach, management and follow-up care[J]. Lipids in health and disease, 2020, 19(1): 2.
[14] RYAN H M, SHARMA S, MAGEE L A, et al. The Usefulness of the APACHE Ⅱ Score in Obstetric Critical Care: A Structured Review [J/OL]. Journal of obstetrics and gynaecology Canada, 2016,38(10):909-918.
[15] KARNAD D R, LAPSIA V, KRISHNAN A, et al. Prognostic factors in obstetric patients admitted to an Indian intensive care unit[J].Critical Care Medicine, 2004, 32(6): 1294- 1299.
[16] YI H Y, JEONG S Y, KIM S H, et al. Indications and characteristics of obstetric patients admitted to the intensive care unit: A 22-year review in a tertiary care center[J]. Obstetrics and Gynecology Science, 2018,61(2): 209-219.
[17] MUENCH M V, BASCHAT A A, MALINOW A M, et al. Analysis of disease in the obstetric intensive care unit at a university referral center: a 24-month review of prospective data[J]. The Journal of reproductive medicine, 2008, 53(12): 914-920.
[18] 刘慧姝 , 王沂峰 , 徐仲 , 等 , APACHE Ⅱ评分在综合 ICU 产科危重患者中的应用 [J]. 2005, 6(6): 428-431.
关注SCI论文创作发表,寻求SCI论文修改润色、SCI论文代发表等服务支撑,请锁定SCI论文网!
文章出自SCI论文网转载请注明出处:https://www.lunwensci.com/yixuelunwen/46546.html